The Science Behind CO₂ Lasers for ENT Procedures
CO₂ lasers deliver this combination because their physics align with the needs of soft-tissue work: a 10,600 nm wavelength that water absorbs efficiently, stable beam profiles, and predictable thermal effects.
This article explains the scientific principles underlying CO₂ lasers and how they support controlled ablation in ENT procedures.

What Makes a CO₂ Laser Unique? Understanding the Physics
A CO₂ laser is a type of gas laser, meaning its gain medium is a mixture of gases, primarily carbon dioxide (CO₂), nitrogen (N₂), helium (He), and often small proportions of hydrogen or xenon.
When the laser is powered on, an electrical current runs through this gas mixture. That energy pushes the nitrogen molecules into a higher-energy “vibrating” state. Nitrogen is good at holding this energy, and it transfers it to CO₂ molecules when they collide.
Once the CO₂ molecules receive that energy, they eventually drop back down to a lower energy state. As they do, they release light, specifically, infrared light at wavelengths of about 10.6 µm and 9.6 µm.
The important thing isn’t just that the light is infrared, but how it comes out. It’s:
- Coherent: All the light waves line up together
- Monochromatic: It’s basically one pure color (one wavelength)
- Collimated: The beam stays tight and doesn’t spread out much
These qualities allow the beam to be focused to a very small spot with predictable behavior, which is essential for surgical work.
The 10,600 nm wavelength is the real reason CO₂ lasers are so effective in soft tissue. Water absorbs this wavelength extremely well. And since human soft tissue is mostly water, the laser energy doesn’t sink very deep. It gets absorbed almost instantly at the surface.
When that absorbed energy is converted to heat, the water in the tissue vaporizes, allowing surgeons to cut or remove tissue with very fine control. Because the beam doesn’t travel far into tissue, it minimizes unintended damage beneath the surface.
How CO₂ Laser Energy Interacts With Tissue
When water molecules in tissue absorb light at 10,600 nm, the absorbed energy rapidly converts to heat. Once intracellular and extracellular water reach vaporization temperature, cells rupture, and the tissue is removed.
This is the core ablation mechanism described in multiple studies that evaluated ablative depth and thermal effects in porcine soft tissue across CO₂ laser power ranges.
Key parameters affecting tissue response include:
Ablation Depth
The optical penetration depth for a CO₂ laser is extremely shallow, often in the tens-of-micrometers range. One study measured approximate penetration depths of ~17 µm in hydrated soft tissue. This allows sub-millimeter control during surgery.
Thermal Coagulation
Immediately beneath the ablation zone, tissue reaches temperatures between 60 and 100 °C, resulting in a narrow coagulation layer. This layer seals microvasculature and stabilizes the surgical margin.
Limited Lateral Thermal Spread
Strong surface absorption and rapid heat dissipation keep the heat zone contained. This property is essential in ENT regions where structures lie close together, and damage margins must be extremely tight.
Components of a CO₂ Laser System
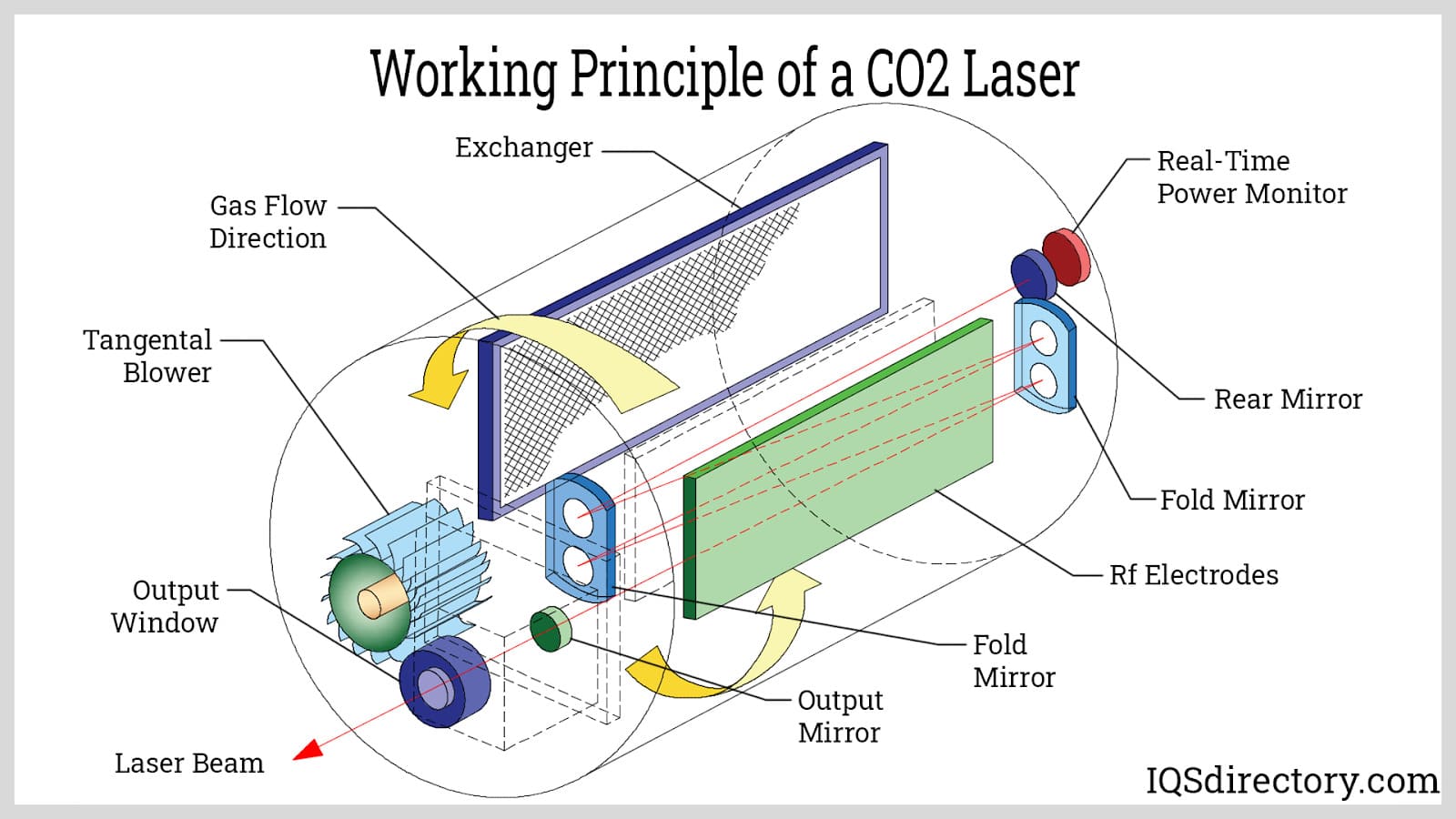
Image source: IQSdirectory.com
A medical CO₂ laser system typically includes:
- Gas-discharge tubes: Multiple parallel tubes hold the CO₂/N₂/He gas mixture. A DC electrical discharge runs through each tube, exciting the gas and producing the population inversion needed for laser emission.
- DC electrodes: Electrodes positioned along the tubes apply the electrical energy that drives the discharge. This energy excites nitrogen molecules, which then transfer vibrational energy to the CO₂ molecules.
- Fold mirrors: A series of precisely aligned mirrors “fold” the optical path into a compact layout. This allows a long resonant cavity without requiring a physically long device. The laser beam bounces between these mirrors as it amplifies.
- Rear mirror and output mirror: These two mirrors form the resonant cavity. The rear mirror reflects nearly all the light back into the cavity. The output mirror allows a controlled portion of the amplified light to exit as the usable laser beam.
- Gas inlet and outlet system: Fresh gas mixture enters through the gas inlets, and spent gas exits through the gas outlets. Continuous flow maintains gas quality, stabilizes output power, and ensures consistent lasing efficiency.
- Laser beam output: After amplifying along the folded optical path, the coherent beam exits through the output mirror as a focused, collimated infrared beam at 10.6 µm.
- A delivery mechanism: An articulated arm or waveguide/handpiece to bring the beam to the surgical site with precise control.
- A delivery mechanism: An articulated arm or waveguide/handpiece to bring the beam to the surgical site with precise control.
Why CO₂ Lasers Are Ideal for ENT Procedures
The synergy between CO₂ laser physics and soft tissue behavior delivers distinct advantages for ENT and similar microsurgical applications:
| Scientific Principle | Practical Benefit in ENT / Soft Tissue Surgery |
|---|---|
|
Strong absorption at 10,600 nm by water |
Highly efficient ablation of water-rich soft tissue and minimal effect on non-water chromophores such as pigment or bone. |
|
Very shallow penetration depth (~10–20 µm) |
Sub-millimeter control of incision depth is ideal for mucosal tissues, vocal folds, or other delicate structures. |
|
Thermal confinement and minimal lateral heat spread |
Clean cuts with minimal collateral damage, less carbonization, and precise margins. |
|
Formation of a thin coagulation layer below the ablation zone |
Instant hemostasis, sealing small blood vessels, reducing bleeding, and maintaining a clear surgical field. |
|
Beam deliverable in pulses (CW, gated, pulsed, super-pulsed) |
Flexibility to tailor energy delivery: fine control when required, deeper ablation when needed.
|
Because ENT work often involves small, delicate, water-rich structures such as mucosa, folds, and microanatomy, CO₂ lasers’ physics align well with clinical demands.

Advances and Engineering Innovations in CO₂ Laser Design
CO₂ laser design has evolved steadily over the past two decades to make today’s systems far more precise, stable, and controllable. Several innovations stand out:
More Sophisticated Pulse Delivery
Early medical CO₂ lasers often relied on continuous-wave energy, which was effective but generated sustained heat in tissue. Modern systems use pulsed and super-pulsed modes that break the energy into extremely short bursts. These short bursts deliver:
- Higher peak power to vaporize tissue cleanly
- Lower overall heat load because the tissue has time to cool between pulses
- Sharper ablation edges with less carbonization
Peer-reviewed studies show that pulse duration and peak power significantly influence thermal spread. Super-pulsed modes, in particular, improve spatial precision because they remove tissue faster than heat can diffuse sideways.
Optimized Beam Quality through Advanced Optics
Reliable ENT surgery depends on a beam that behaves the same way every time. This requires a consistent beam shape, stability, and alignment. Modern CO₂ systems improve beam quality by:
- Applying high-reflectivity mirror coatings designed for the mid-infrared spectrum
- Using optical materials with superior transmission at 10,600 nm (e.g., high-grade ZnSe or diamond optics)
- Minimizing internal losses so the beam exits with uniform energy density
These improvements produce a beam that is both homogeneous and predictable, helping avoid hot spots and allowing surgeons to use smaller, more precise spot sizes without introducing irregular thermal effects.
Refined Spot-Size Control and Delivery Systems
Spot size determines how energy concentrates in tissue. A smaller spot means more energy per unit area and finer surgical detail. Engineering advances now allow:
- Sub-millimeter spot sizes optimized for microsurgery
- Stable focusing assemblies that maintain spot geometry even at challenging angles
- Improved articulated arms with better mirror alignment and smoother mechanical travel
- Handpieces and waveguides designed specifically for ENT ergonomics
This level of control is especially important in regions such as the vocal folds, nasal cavity, and airway, where even a slight change in spot diameter changes the thermal footprint.
None of these engineering upgrades replaces the basic physics of CO₂ lasers. The strong absorption at 10,600 nm remains the core advantage. What modern engineering does is increase the surgeon’s ability to wield that wavelength with consistency and a high degree of reproducibility across procedures.
Understanding the Science Behind CO₂ Lasers Enhances Surgical Confidence
For surgeons, biomedical engineers, and procurement teams, it is critical to look past marketing and focus on the scientific foundation of CO₂ lasers. The 10,600 nm wavelength, high water absorption, shallow penetration depth, and predictable thermal behavior combine to create a tool that is precise, controllable, and suited for delicate soft-tissue work, especially in ENT.
Engineering refinements such as pulsed emission, improved optics, and refined beam delivery enhance the technology, but the core remains the physical laws. Awareness of those laws and their limitations allows users to select systems, plan procedures, and operate safely and effectively.
At IML, we believe that surgical technology decisions should rest on clear scientific understanding. A laser system is not “good” because of branding. It’s good because of beam physics, tissue interaction, and engineering quality. Feel free to explore our CO₂ laser category pages or reach out for detailed technical support.